
It is an hornor and my great pleasure to give the special lecture of the 40th Annual Meeting Korean Society for Preventive Medicne and I also wish to thank you chairman, Dr.Lee for his kind introduction.
The lecture I am presenting is about epidemiological findings on hypertension in our studies which is carried on during around 35 years in our Department of Hygiene Hirosaki University School ofü@Medicine, including some aspects ofü@the relationship between daily salt intake and hypertension, and also I would like give the recent information on the results of the intervention for the prevention of stroke and hypertension in Japan.
First slide is the reprint of the paper which is presented by Dr.L.K.Dahl on the possible role of salt intake in the development of essential hypertension in the international symposium on hypertension held at Berne in1960.

In the symposium he reported the evidence the salt ingestion may be related to human hypertension based on the results of the epidemiological studies, including the data ofü@Japan., in the figure on the correlation of daily salt intake with prevalence of hypertension in different geographic areas and among different races.
This slide shows the distribution of death rate per 100,000 males aged 30-59 years from cerebral hemorrhage in varoius regions of Japan and average daily salt intakes of farmers in 4 regions added to original papers which we reported in Human Biology in 1957.
This is the first scene of our epidemiological studies on stroke and hypertension carrying instrumentsü@for the determination ofü@blood pressure on the trailer and visiting farmers in their homes from door to door.
We started epidemiological studies on stroke and hypertension, especially in the inhabitants of the Northeast Japan in 1954.
ü@At that time there was no definite explanation has been given for the fact that stroke is so common in Japan, and also there was no data on blood pressure of the population except the data of patients in clinics or the data from life insurance applicants.
First we collected the data of mortality from stroke by descriptive epidemiological studies.
As regards the death rate from stroke in Japan there exist a couple of distinguishing features.
The first one is that there is throughout the country a marked geographical difference in the death rate.
The second one is seasonal variation, this being low in summer and high in winter.
The third one is decline in the death rate from stroke during the periods World War II.
It appears likely that these above-mentioned characteriscs can be the best clues to the epidemilogical research for the explanation into the nature of stroke or hypertension considered to underlie it.
Epidemiological studies on hypertension should be started with obsevations on blood pressure of a group of man.
We have made many observations on the blood pressure of the populations in the northeast of Japan by local mass surveys.
I presented the working hypothesis on epidemiological clues to hypertension from a global viewpoint on high blood pressure and its relationship to sodium chloride intakes at the Seminar held at the Laboratory of Phsiological Hygiene School of Public Health Minessota University in 1966 while I was staying as Visiting Professor.
I made a comparison of the daiy salt intake and the blood pressure of populations according to the literature from various parts of the world, and I showed that there is some correration between the two.
Among these reports the blood pressure level appears to be already high in younger group in areas with salt intakes of more than 10 g per day for a person, with subsequent rise of blood pressure upon aging and in area with salt intake of less than 5 g on the other hand, the blood pressure level was low at a younger age and no rise noted with advance in age.
The blood pressure of humans varies from a low level with a narrow range of a natives of Brazil and New Guinea, to high level with a wide distribution beginning with childhood and progressing with age to a higher level and wider distribution just as the inhabitants of Northeast Japan.
I presented this findings at the round table session entitled Causative Factor in Hypertension in the 6th World Cpngress of Cardiology held at London in 1970.
But these findings were based on the data from crossectional epidemilogical studies and the technique for the determination of blood pressure and methods for the determinations of daily salt intake were not consistent as a whole.
So we are trying to make one useful method in the epidemilogical study on hypertension as Objective Recording Method.
One instrument based on this ideas is used for the determination of blood pressure in the epidemilogical study of WHO CARDIAC Study.
And we can analyse the data of Korotkov sound in the tape recorder by ordinary micro-computer and can get completly objective proof of the blood pressure.
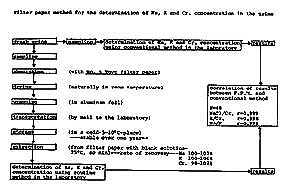
Concerning to the determination of daily salt intake we have developed a new method for the determination of urinary sodium, potassium and creatinine. We named the new method as Filter Paper Method, FPM.
The detail of the method of Filter Paper Method is shown in the Fig.1.ü@ We have made many observation on urinary output of salt from the various parts of the world until now.
According to the longitudinal epidemiological studies on hypertension the blood pressure of population was determined once or twice a year by mass surveys from 1954 up to 1975.
The transition of the personal blood pressure of the population and the mean blood pressure level of the population to the northeast Japan from 1954 to 1975 are calculated by regression analysis of the data obtained during the entired periods. The number of person determined in the population of the northeast Japan was 1127 for males and 1367 for females. The response rate was 98.5 percent and the average times of determination of blood pressure by mass survey during the entire periods for a person was 12.9.
The birth cohorts as established in the 1967 except the person moving in or out during entire periods were followed by death certificate to identify deaths occuring in subsequent years up to 1975. Person years of observation is used for calculating death rates in cohort stydy especially in the death rate from stroke at every 10mmHg level in the distribution of blood pressure. According to the results obtained in this study it become obvious that a person whose blood pressure levels was high from the younger age are apt to get attack to death from stroke and that person whose blood pressure were aound 120 mmHg for the systolic blood pressure and 70 mmHg for the diastolic blood pressure were lowest in the death rate from stroke.
And the death rates from stroke showed "smooth" increment in the same propotion as the rise of systolic and diastolic blood pressure levels in the order of cerebral hemorrhage and cerebral infarction and others in semi-log scale figure.
For the explanation of the presense of various chracteristic in the mortality from stroke and in the blood pressure levels and its transition of the population we got the clue, that is, the quantity of salt intake which was influenced by long standing eating habits from the childhood, is the most influential factor from our studies.
We have made an attempt to demonstrate the change in salt intake and blood pressure for the same person during the past 20 years. Three consecutive 24-hour urine samples were collected from the same person in 1961 and 1981. Blood pressure was determined once or twice a year by mass survey and the levels and changes in the blood pressure for each person were calculated according to the records obtained during the entire periods. The salt intake of farmers in the northeast Japan decreased from 17.0 g per day in 1961 to 11.9 g in 1981 and the blood pressure did not rise with advance in age during the past 20 years.
And on the whole the correlation between the average levels of blood and the salt intake. The fact that the mortality from stroke and the blood pressure were comparatively low in the apple producing regions in the northeast Japan suggesting that eating apples containing abundant potassium, may have something to do this phenomenon and emphasized the necessary to give consideration to balance between sodium and potassium in the daily dietary life in the paper entitled High Blood Pressure and the Salt Intake of the Japanese in 1962.
According to the results obtained in the longitudinal epidemiological studies we could get some relation between apple eating habits and in the transition on the personal blood pressure levels when we divides by eating habits at the time of the first 1958 periods.(Fig.2.)
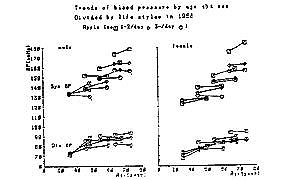
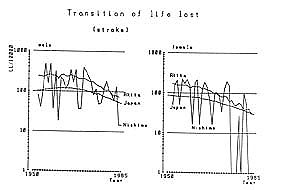
Fig.3 shows the recent findings in the transition of death rates from stroke in Nishime-village, Akita prefecture and all Japan.These lines show the transition of life lost from stroke.
The values of life lost are different from so-called crude death or standardized death rates. The value of life lost shows the lost of the potential or working year under 70 years.
In Japan the amounts of daily salt intakes decreased from aound 17 g to 12 g for a person per day during the past 30 years according to the results of National Nutrition Survey, especially after the recommendation on the modernization of the marketing system of food with a view to a systematic improvement of the nation food life from the Science and Technology Agency of the Japanese Goverment in 1965 which is the recomendation on the change of the method of preservation of food from salt to refrigeration.
In a farm village, Nishime in Akita prefecture in the northeast Japan, we conducted the intervention for the prevention to the hypertension and stroke from 1957. The hypertension control measure was formed of the improvement of dietary conditions such as a high intake of salt and the improvement of the way to live through winter in a warm manner. According to the results of intervention studies on the hypertension control the levels and frequency distribution of blood pressure and the way of living such as traditional high salt intake in the inhabitants of northeast Japan not only in a middle age group but also in such a young group as middle school children and the decline in the values of life lost from stroke in Nishime village was observed in recent years.ü@ü@